Joint hypermobility exists across a broad spectrum and is found in both active and general populations. It refers to joints that move beyond expected physiological ranges because of differences in connective tissue properties, joint structure, and passive restraint systems. Some individuals present with generalised hypermobility throughout multiple joints, while others display increased motion only in selected regions such as the knees, shoulders, ankles, or spine.
Research shows that occurrence rates vary according to age, sex, ethnicity, activity level, and the criteria used for assessment. In many populations, younger individuals and women demonstrate higher rates of generalized hypermobility, although this is not consistent in every cohort. Joint mobility also tends to decrease with age as connective tissues undergo structural remodeling and become less elastic over time, according to recent research on age related changes in collagen and elastin properties.
From a movement perspective, hypermobility is not simply increased flexibility. Greater passive range often means the surrounding musculature must provide more dynamic support during standing, walking, lifting, and sport. Where one joint gains stability from ligament tension and capsular restraint, another may rely more heavily on muscular control and coordinated movement patterns.
This has mechanical consequences. Increased stabilizing demand may contribute to fatigue, persistent muscular tightness, reduced tolerance to prolonged standing, and overload symptoms during repetitive tasks. The sensation of tightness in hypermobile individuals often reflects protective muscular tension rather than a true lack of mobility.
Many individuals remain symptom free. Others begin to experience pain in early adulthood, particularly when training load, occupational demand, previous injury, deconditioning, pregnancy, or prolonged stress exceed the body’s ability to maintain control and recover effectively. Age alone does not exclude meaningful joint symptoms in a hypermobile system.
Common complaints associated with hypermobility include recurrent ankle sprains, anterior knee pain, patellar irritation, shoulder instability, lumbar discomfort, neck tension, pelvic asymmetry, and diffuse soft tissue soreness. These findings are not exclusive to hypermobility, but increased joint motion can be one contributing factor.
There is also growing interest in the relationship between hypermobility and early degenerative joint change. Hypermobility does not automatically lead to arthritis, and many individuals never develop significant degeneration. However, excessive joint motion, recurrent instability, altered load distribution, and previous injury may increase long term wear in selected joints. The knee, hip, thumb base, and shoulder are commonly discussed areas, while spinal symptoms may relate more to mechanical irritation than degeneration alone.
Hypermobility should therefore be viewed as a risk modifier rather than a direct cause of arthritis. Body weight, muscle strength, occupational load, previous trauma, genetics, and overall activity history remain major influences on joint health.
This is where generic exercise approaches often fail. Two people may both present with knee pain, yet one requires restoration of lost mobility while another requires improved strength, deceleration control, and frontal plane stability. Applying the same program to both ignores the underlying mechanics.
The same principle applies elsewhere. A hypermobile lumbar region may benefit more from trunk strength, endurance, and load management than repeated stretching. A hypermobile shoulder often responds better to scapular strength, rotator cuff conditioning, and controlled loading than attempts to gain further range of motion.
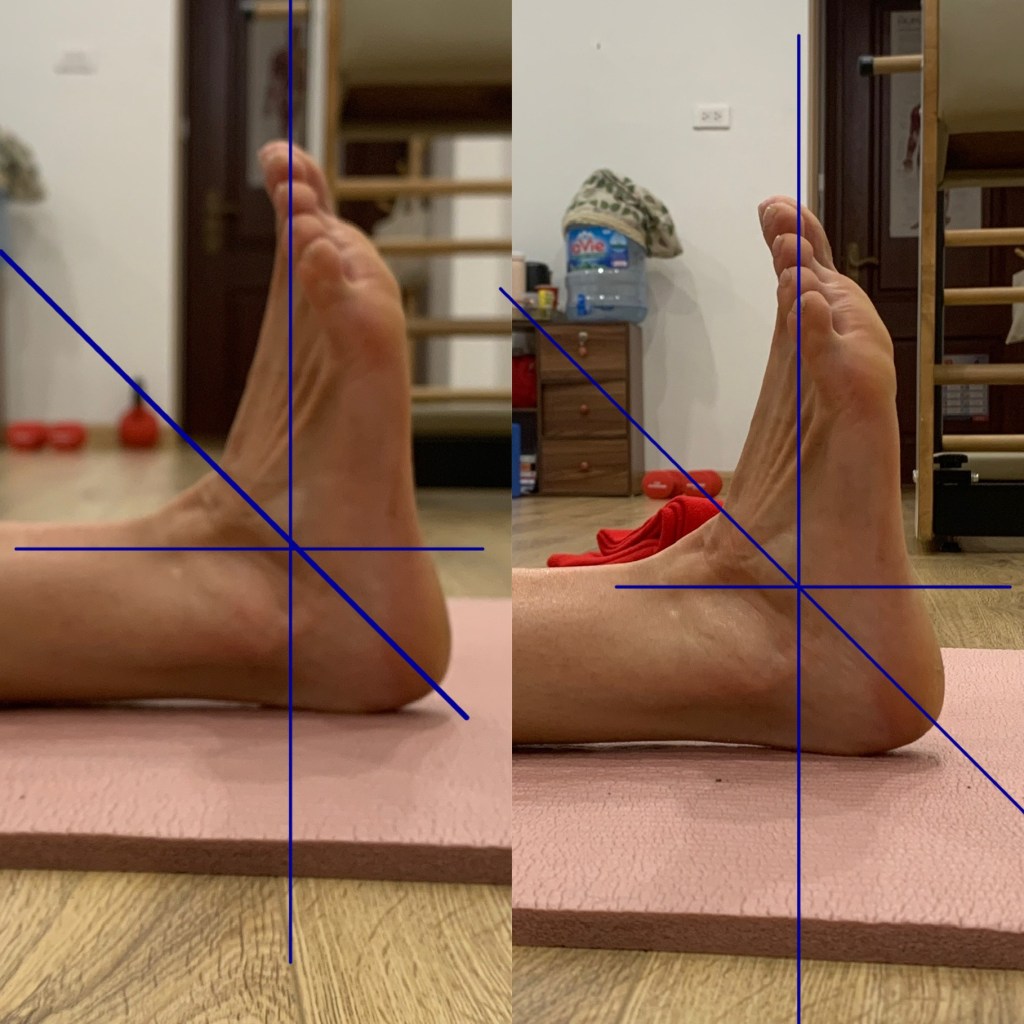
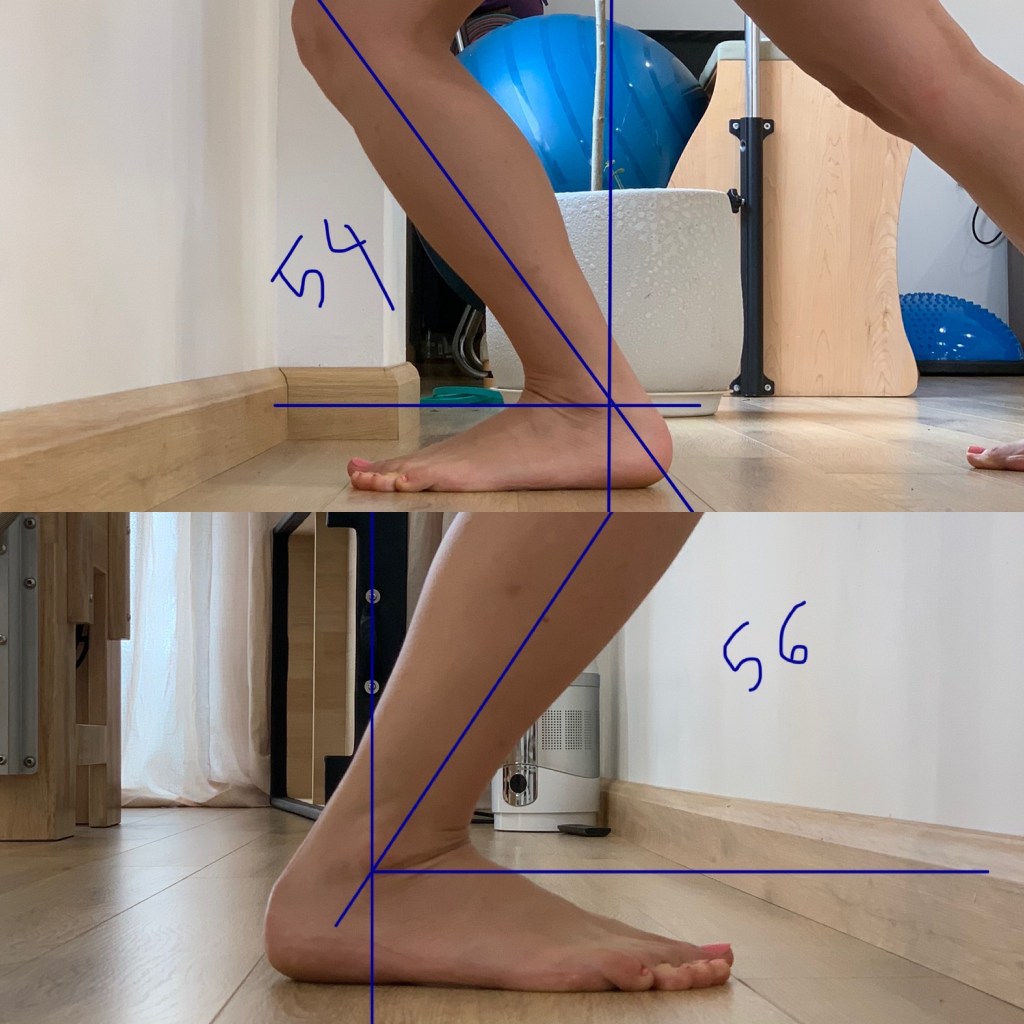
Human anatomy follows common patterns, but skeletal geometry, femoral version, tibial torsion, acetabular orientation, foot structure, tissue stiffness, and movement strategies differ considerably between individuals. Neutral alignment should therefore be viewed as a functional range rather than one universal position.
When symptoms are present, evidence generally supports active management. Progressive resistance training, balance work, proprioceptive retraining, graded loading, and movement education are often more beneficial than passive treatment alone. The objective is not to eliminate mobility, but to improve control, capacity, and tolerance to load.
Joint hypermobility is not inherently pathological. It is a physical trait that may offer advantages, create challenges, or remain irrelevant depending on the individual and the demands placed upon the body. Effective management depends on accurate assessment, appropriate loading, and recognition that not all joints require the same strategy.
References
Castori M, Tinkle B, Levy H, et al. A framework for the classification of joint hypermobility and related conditions.
Remvig L, Jensen DV, Ward RC. Epidemiology of general joint hypermobility and basis for the proposed criteria.
Juul-Kristensen B, Schmedling K, Rombaut L, Lund H, Engelbert R. Measurement properties of clinical assessment methods for generalized joint hypermobility.
BMC Sports Science, Medicine and Rehabilitation. Resistance training in women with generalized joint hypermobility: randomized controlled trial.
BMC Musculoskeletal Disorders. Generalized joint hypermobility and associations with musculoskeletal symptoms and quality of life.
International Consortium publications on hypermobile Ehlers-Danlos syndrome and hypermobility spectrum disorders.